What do you think the chances are of knowing:
1) Someone who used to work with an angry man --- > woman, gender changed, transvestite?
2) Someone who was laid off for not being able to work in a lab with a leaking chemical tank with said transvestite?
3) Someone who found out her Mother has cancer 30 mins after she got laid off, the same Mother that "hid" her years earlier cancer Dx?
As I was leaving the cancer center for the last time as an employee this afternoon, I ended up sitting on the shuttle next to a middle aged woman, with the body of a 20 year old. Fo' real! And she was talking about the treatment she was getting for her stage IV thyroid cancer. And I was once again reminded that while the road ahead for my Mother is filled with uncertainty, today we're here and doing our best to deal with the here and now. I was also reminded that God himself has removed a TREMENDOUS burden/obstacle for me being able to be there for my Mom in the next how ever many months. And I know His grace and mercy will see me through.
Ironically, I'll be back at the cancer center in 2 weeks for a required rotation for my Health Informatics class which just happens to be in the same department I was laid off from. And I also have an interview with 2 PI's about research projects in the department down the hall.
Oh well, "on to da' next one"!!!!
Monday, March 31, 2014
Sunday, March 30, 2014
Get busy livin' or get busy dyin'
One of the my favorite movie quotes from Shawshank Redemption is the title of this post. And it's such a personal reminder that unfortunately, I spent much of the last 10 or so years of my life getting to a goal, instead of enjoying the journey on the way. Yeah I know, it sounds sooooo cliche', but very true in my case. And through a TON of soul searching I learned to really L-I-V-E my life instead of just letting life pass me by.
Along those same lines, here's a picture of me and one of my sista' mentors, Dr. E who recently went on to greener pastures after working with me at the Cancer Center where I'm currently employed:

Before getting together with Dr. E and a couple other female Scientists and Clinical Lab profesisonals, I'd seen 2 clients, attended an open house at another university that's throwing a LOT of money my kid's way, and cooked a few of my favorite southern treats to serve the ladies at our gathering. In other words, those bags under my eyes were VERY well earned LOL, but I was DE-TERMINED not to let that keep me from enjoying the evening. And enjoy it I did along with picking up another client for my business!
Of course all this running around caught up with me this morning and I didn't get out of bed until after 9 this morning which is MUCH later than my 5AM regular wake up time. But I know I needed the rest because in addition to the homework I have to do for my Bioinformatics course today, I have 2 clients to see today as well.
But it's all good, because I'm "livin' my life like it's golden" and "golden" it is!!!
Along those same lines, here's a picture of me and one of my sista' mentors, Dr. E who recently went on to greener pastures after working with me at the Cancer Center where I'm currently employed:
Before getting together with Dr. E and a couple other female Scientists and Clinical Lab profesisonals, I'd seen 2 clients, attended an open house at another university that's throwing a LOT of money my kid's way, and cooked a few of my favorite southern treats to serve the ladies at our gathering. In other words, those bags under my eyes were VERY well earned LOL, but I was DE-TERMINED not to let that keep me from enjoying the evening. And enjoy it I did along with picking up another client for my business!
Of course all this running around caught up with me this morning and I didn't get out of bed until after 9 this morning which is MUCH later than my 5AM regular wake up time. But I know I needed the rest because in addition to the homework I have to do for my Bioinformatics course today, I have 2 clients to see today as well.
But it's all good, because I'm "livin' my life like it's golden" and "golden" it is!!!
Friday, March 28, 2014
Who's "got you"?
Reflecting on the mean ass, triflin' message left by an anonymous poster the other day reminded me of how absolutely critical it is for super nontrads (premeds over age 40) to have their support systems SUPER in tact.
Then I got to thinking about the numerous people who were in my life say 3 years ago, that no longer are. Or as in the case of my mother, folks who I just don't discuss details of my career plans with (which makes me really miss my Dad, because there was nothing in the world he didn't think I could do). Luckily for me, my support system is more in tact now that it has EVER been but I've had to adjust to a few things, because while it used to be easy for me to find mentors, the older I got, the harder finding supportive mentors became. And as much as I'd like to think my age isn't playing a HUGE factor in that, the fact is that I think it is primarily due to my MD/PhD goal.
Movin' on, my business is now really booming as in I'm almost making the same salary from my "real job", but working only 1/4 of the time. Yeah! :)
I also learned that I won't be able to start my fellowship until May or August of this year. And that's kinda sad but I think it means that there's more God wants me to learn where I'm at right now. So I've come to terms with that and I'm enjoying my current gig more than ever now that I understand why I'm here. Learn the lesson, then move on.
Class wise things are fabulous, I've got a 100% average in the second part of my Bioinformatics methods course and I've scheduled my ER and second IM clinic rotations for my Health Informatics course. My R programming course starts in a week and I have NO idea how I'm going to be able to do it all, so I may just drop that class depending on if I get a definitive start date on my fellowship.
Now I'd like to end this post with my favourite song by the group The Roots featuring my other girl, Eryka Badu. Because I know without equivocation that there are many people, both in my personal and professional life, "who've got me"!!!
Then I got to thinking about the numerous people who were in my life say 3 years ago, that no longer are. Or as in the case of my mother, folks who I just don't discuss details of my career plans with (which makes me really miss my Dad, because there was nothing in the world he didn't think I could do). Luckily for me, my support system is more in tact now that it has EVER been but I've had to adjust to a few things, because while it used to be easy for me to find mentors, the older I got, the harder finding supportive mentors became. And as much as I'd like to think my age isn't playing a HUGE factor in that, the fact is that I think it is primarily due to my MD/PhD goal.
Movin' on, my business is now really booming as in I'm almost making the same salary from my "real job", but working only 1/4 of the time. Yeah! :)
I also learned that I won't be able to start my fellowship until May or August of this year. And that's kinda sad but I think it means that there's more God wants me to learn where I'm at right now. So I've come to terms with that and I'm enjoying my current gig more than ever now that I understand why I'm here. Learn the lesson, then move on.
Class wise things are fabulous, I've got a 100% average in the second part of my Bioinformatics methods course and I've scheduled my ER and second IM clinic rotations for my Health Informatics course. My R programming course starts in a week and I have NO idea how I'm going to be able to do it all, so I may just drop that class depending on if I get a definitive start date on my fellowship.
Now I'd like to end this post with my favourite song by the group The Roots featuring my other girl, Eryka Badu. Because I know without equivocation that there are many people, both in my personal and professional life, "who've got me"!!!
Thursday, March 27, 2014
MICU rotation, part 1

I'm pretty sure I'm going to need 2 posts to talk about what I observed in the MICU, it just REALLY blew me away. I didn't have much to say during this rotation, no thoughts on care, because obviously almost EVERYTHING was COMPLETELY over my head! Except, one case of COPD of unknown etiology until I asked about the occupation of the patient. And that happened to be in the chemical industry, so it was no surprise that an illegal immigrant working in a chemical plant, likely without the proper respirator equipment would have full blown COPD with heart failure at the age of 53.
Anyhoo, almost every patient on the floor was on a ventilator. Including a patient whose family I met at the nearby cafe which was on the same floor and around the corner from the MICU. And in the strangest form of irony, this was also the patient that coded while I was in the MICU. I accidentally met the family of the patient when I thought I was lost and was asking people I saw in the area if I were in the right place. The sister of the patient told me that the doctor I was looking for was her sister's doctor and that the doctor was a very nice lady (which she was and REALLY sharp too). I told her that I hoped her sister would have a speedy recovery and she slowly shock her head no then her head dropped down for a second. When she looked up, she had tears in her eyes and she replied that no, her sister probably wasn't going to be OK. And to that I said that I would pray for her sister and family anyway and I reminded her that God has the final say. At that point, it was time for me to report to the MICU.
The first patient I saw was the man with the advanced COPD, followed by a terminal case of squamous cell carcinoma of the throat, a case of cirrhosis of the liver, a brittle diabetic, and finally the sister of the woman I saw at the cafe, a case of AML which had not responded to treatment (As I understand it, AML is the worst Leukemia to have). The AML patient was my age 47, and had been diagnosed 4 months ago. Unfortunately, she wasn't responding well to treatment and had been in the hospital for the past 5 or so days. She was one of the last patients I saw and when I looked in her room, the sister I had seen at the cafe looked at me as if to say hello and I responded by smiling slightly and nodding my head.
Our group was just about done rounding when I heard all kinds of alarms going off and all the doctors in our group headed straight for the room of the patient with AML. Her head was tilted so that it was pointing down which I assumed meant she was having a blood pressure problem but I don't know for sure because I had to leave before rounds ended (I'm going to check with the doctor to see how this patient is doing, our being the same age struck a nerve with me). What I do remember is that she had had problems the night before due to an improperly placed Dobhoff tube causing a pneumothorax. A pneumothorax that was missed by the Resident and caught by the Attending who was none too pleased (Gosh, being a Resident must REALLY be hard). And I could tell the Resident who missed it really cared about the patient, unlike the 5'2", balding Jewish Resident who I overheard calling rounding "a bunch of crap". (He had on a Yamaka which is how I knew he was Jewish, and with Jewish ancestors, I'm comfortable calling his arse out!). I digress, I was happy that the patient's sister had already left when the emergency began but I'm pretty sure she was called back in. When I left, she was stable but her prognosis didn't seem very promising.
The other patient I remember well was a brittle diabetic, a Black woman who not surprisingly, was "very well nourished" and around my age too. In fact, EVERY minority I saw on the floor was overweight, reminding me that minorities really gotta' work on NOT "digging graves with forks". In her case, her diabetes wasn't well managed though I didn't really know why besides the fact that she looked non compliant based on her weight and poorly managed disease though I know the 2 aren't always associated. However overnight, her feedings had been withdrawn for reasons I can't recall. But what I do recall was that she was given 2 units of insulin in a fasting state so needless to say, things weren't looking good for her during rounds the following day. I also recall that this patient was assigned to the balding Jewish guy, and my immediate first thought was that his flippant attitude about rounding seemed to be carrying over into his bedside manner. So my question then became how in the hell did HE get into medical school?
Honestly, these are the kind of situations that have always worried me about going into patient care, what do you do when the person you're rounding with or are in school with seems to not care about what they do? It would be so hard for me to be silent knowing that my silence could cost someone their life, literally. But then I've already lost 2 jobs for not being willing to stand idly by as life threatening decisions are made, such as passing off bad data for a clinical trial. I just pray and I pray REAL hard that God doesn't allow anything like this to happen around me. Because I know if I were the patient, I'd certainly want someone speaking up to save my life.
Wednesday, March 26, 2014
Hey pretty ladies, I think I'll sit between ya'll!

* Image from Google Images
This scene from the Pretty Woman is my absolute in the movie!!
Anyhoo today, I had a LONG day at work and wasn't feeling well, so this was just the pick me up I needed.!! The older man that greeted me and another young lady with "Hey Pretty Ladies......", was with his son who looked to be about my age. And they were at the cancer center getting treatment for his son's leukemia. The man told me that he, his wife, and son had moved to Texas last week and would be here a year, after not being satisfied with the treatments options at Hopkins. His exact words, he didn't feel like the folks there were doing enough.
He was from Annapolis, MD which is not far from where I had lived just last year. We talked about the good places to eat, how much new construction is causing the city of loose it's charm, and how nice the people here in Texas are.
About this time, his ride to the parking garage had arrived and then I felt a lump in my throat. Oh boy, I said to myself, here we go again. It took everything I had to keep the tears from flowing down my cheeks and regular experiences like these are a HUGE part of why working at a cancer center is so hard for me. Add that to the "code" I observed in the MICU earlier today, and I was a tearful basket case (I'll talk more about my MICU experience on a later post). But these are experiences I know God is allowing me to have for a reason, because in the end, I think they will make me phenomenal Physician one day.
Tuesday, March 25, 2014
From Comment to post, March 2014

*3/26/14 - I decided to edit this post because I'm aware more than ever that with all the evil and negativity in the world, I need to put positive stuff out there in the universe that's going to be associated with me.
** 3/27/14- I also decided to edit my song choice too because as aporpos as the Cee Lo Green song is, I think this song by my girl Jill Scott says the same thing with a LOT more class and conviction:
Saturday, March 22, 2014
Patient 2, Internal Medicine rotation

The second patient I saw on IM rounds was a 45 year old Black man who was HIV positive. I can't exactly recall what led to his ER visit, but I remember quite well that his T-cell count was near 0 upon admission. I also remember that the others on the team wouldn't go into his room and while I gathered that he was a difficult patient, it seems VERY strange to me a group of current/future doctors would be "afraid" to go into the room of an HIV positive patient. At least that's how I read it, as fear. I mean if Mr. Jackson was throwing poop at folks when they walked in the room, I could understand "the fear" to some extent. But to me, their fear was just ignorant. You see I was a volunteer AIDS counselor for many years and used to do blood draws for HIV test at a rural public health clinic. So, I figured that since I wasn't planning on having sex with Mr. Jackson, I didn't have anything to worry about.
So I put on the disposable gown and went to visit Mr. Jackson with Dr. B.
The room was very dimly lit and the only other person in the room was Mr. Jackson's daughter. And she was beyond pleasant and thankful to Dr. B for essentially saving her Dad's life. Turns out, Mr. Jackson had a BIG problem with taking pills and I surmised that after almost 20 years of being HIV positive, he had grown weary of taking lots of pills everyday. So Dr. B had ordered a Hospice consult for Mr. Jackson not out of need per se, but to "encourage" Mr. Jackson to take his medication. And immediately after the hospice folks left, Mr. Jackson started taking his HIV meds. The day of our visit, his T-cell count was almost back to normal and Dr. B was checking in on how he was doing.
What I learned that day was that despite CLEAR evidence for how HIV is likely transmitted, people are STILL ignorant about it. And to see medical folks behave out of fear was mind boggling. I mean, all one student did was touch the door handle of Mr. Jackson's room and he disinfected his hands immediately after he let it go. And no, I didn't see him do the same with ANY other patient we saw that day.
Again, ALL I could think about was how what I saw that day rounding emphasizes the need for both more compassionate and minority Doctors. I also thought that my personal argument for why no one under age 25 should be admitted to med school was substantiated as well.
Friday, March 21, 2014
Yes!!!
Yesterday, I unofficially became a Predoctoral Fellow in Health/Biomedical Informatics at a major university. And my career in cancer isn't over either, I'll be studying cancer drugs which brings into serious play, my background in pharmacology and chemistry. Talk about a mixed bag project!!! Right now, my new PI is working on the "semantics" of the gig since it was advertised as a Post Doc position and that may take a little time. Needless to say, I'm pretty excited about combining most of what I've learned academically into the foundation of my dissertation!!
So the goal is to over the next 2 years, complete the remaining courses I need for the PhD, pass my cums and orals (that's PhD slang for cumulative and oral exams, let's keep it clean folks), then matriculate in medical school. How do I plan to finish PhD research while in med school? By busting my tail during the summer before med school and the one following first year. And because I've already taken most of the first year med school curriculum and have tutored in many of the subjects since then, I think I'll be able to put at least 20hrs/week toward my research project. Obviously, none of this is set in stone, but this is the plan today. And it's a plan I've waited a VERY long time to see come to fruition!!
So the goal is to over the next 2 years, complete the remaining courses I need for the PhD, pass my cums and orals (that's PhD slang for cumulative and oral exams, let's keep it clean folks), then matriculate in medical school. How do I plan to finish PhD research while in med school? By busting my tail during the summer before med school and the one following first year. And because I've already taken most of the first year med school curriculum and have tutored in many of the subjects since then, I think I'll be able to put at least 20hrs/week toward my research project. Obviously, none of this is set in stone, but this is the plan today. And it's a plan I've waited a VERY long time to see come to fruition!!
Wednesday, March 19, 2014
Patient 1, Internal Medicine rotation.

* Image from Google Images
**While the following case is based on a true patient, the true identity of the patient has been changed in the interest of privacy.
Dr. B: "Kimberly, how good are your powers of persuasion"?
I knew as soon as Dr. B asked this question I was once again being tasked with talking to a patient with serious medical "issues". Ironically, the exact same thing used to happen over 25 years ago when I volunteered at a rural health clinic. Why folks seem to think I'm skilled in this area I don't know, but I like a challenge, so I accepted not being sure of what I was agreeing to.
Doc201X: " I think I'm pretty persuasive...........hang on, what am I agreeing to?"
Dr. B: "Thank you Kimberly, you've just volunteered to talk our 400 pound patient into getting out of bed twice a day."
And with that he proceeded to give us the clinical presentation of Mr. Hernandez as we surrounded him at the "cart".
Dr. B: "Mr. Hernandez is a 450 pound well nourished Hispanic male, whose chief complaint upon admission to the ER was severe back pain. After an X-Ray, it was determined that Mr. Hernandez has a compressed spine likely due to his excessive weight. Kimberly, we've been trying for almost a week to get Mr. Hernandez to get out if bed, do you have any ideas"?
Doc201X: "Sure......Maybe, but I'll give it a shot anyway!".
As soon as I took one long survey of Mr. Hernandez's extra large bed with a mini crane looking attachment, I immediately identified the problem with Mr. Hernandez getting out of bed.
Dr. B:"Buenas Dias, Señor Hernandez, como' estas?"
Doc201X: "Buenas Dias, Señor Hernandez."
Mr. Hernandez: "Something in Spanish I did NOT understand".
I immediately looked at Dr. B in utter confusion because while my Spanish is pretty good, I can't understand a lick Mr. Hernandez is saying because Mr. Hernandez has NO teeth.
Dr. B: "Lo siento señor Hernández. ¿Ha tratado de salir de la cama hoy?
Mr. Hernandez: "No, mi espalda todavía me duele mucho. Y me caí de la cama cuando trataba de ponerse de pie."
Doc201X: "Perdone, pero no entiendo porque estás hablando muy rápido". Habla mucho despacio por favor."
He repeates himself slower this time.
Doc201X: "Lo seinto, señor. ¿Te gustaría una cama más baja?"
And with that, Mr. Hernandez's problem may have been solved. He was about 5'3" tall and his VERY large bed looked about 2 feet off the ground. So with him being so large, he would practically fall out of bed trying to get out of bed, hence his reluctance to get out of bed. DUH!!!
The assumption of the team had been that Mr. Hernandez was just being lazy. Which may have been true to some extent, but how no one noticed how high the bed was off the floor and how short/large he was in realtion to it, still boggles my mind when I think about it. I get why the Doc could have overlooked this because he has a thousand other patients to think about. But for the others to joke about the guy and write him off as lazy just rubbed me the wrong way. So after finishing up with his patient record and discussing what they knew of his life and history, it occurred to me to ask if a Psych eval had been done on him. The team looked perplexed by the question, but Dr. B asked me why I thought it was necessary. I responded that no one I know wants to be 450 pounds and given what we had discussed about his history of using the ER as a primary care facility and other family/medical issues, that perhaps he needed a Psych eval. Dr. B mulled it over for a second, then ordered the Psych eval.
Clinical medicine, here I come!
I almost forgot to mention that I'm interviewing for a Bioinformatics Informatics fellowship tomorrow!!!
Friday, March 14, 2014
At a lost for words!
* Image from UA med school

And that pretty much sums up my half-day rounding in IM at the local county hospital. Absolutely AMAZING, clinical care here I come!!!
Man, where do I begin? I'll start with the obvious; the serious patient risks of not having culturally competent Doctors costs lives, absolutely NO doubt about it! Not only were half of the patients I saw Spanish speaking, they were mostly minority, which probably doesn't come as a surprise considering that most of their funding is from Medicaid/Medicare. So I got a chance to brush off my Spanish speaking skills and my ebonics skills too, LOL!! Honestly, if the Doctor can't communicate with the patient because the translator can't be everywhere at the same time, how in the hell can they effectively provide care?
Anyhoo, during rounds I suggested ordering a Psych eval, thyroid panel, hormone status ie menopause, and a couple other things. And what became glaringly obvious not just to the team that I rounded with but the Attending as well, is that my life, educational, and professional experiences puts me FAR ahead of the average med school applicant in terms of just knowing what to do when what to do isn't obvious. I also think my ability to relate culturally helped too. Sure, my group had me "beat" in many of the clinically obvious things because this is what they've been doing full-time for the last 3 to 5 years. But those basic or gut instinct skills that typically come with age/wisdom, they just didn't have because they haven’t been around long enough or had enough life experience to know anything different. And this is the point older premeds need to emphasize in interviews. All that said, Dr. B my Attending, who's also the professor for my healthcare course, not only speaks fluent Spanish, he's got compassion "on lock". There wasn't ONE patient he didn't easily communicate with and I think that speaks to the kind of person/Doctor he really is.
I almost forgot to mention the computer cart AKA point of care cart, Dr. B used to both review and immediately enter patient data into the EPIC EHR, an image of which is shown below:

Again, I was TOTALLY AMAZED, I had finally seen the EPIC EHR in action in a real life medical setting and it's honectly not as bad as MANY Docs say it is. So the way our rounds worked, is that Dr. B gathered us all around it to discuss the patient, look at labs, xrays, ect. The monitor appeared ot be about 27'. Then we would go see that patient, ask them how they were doing, any complaints, ect, then we returned immediately to the cart to enter the pertinent data. Again, VERY cool!
So after giving me kudos for thinking of differentials on patients that neither he nor the team had thought of, I told Dr. B that I was taking the MCAT in the fall and applying to med school. At almost 50 years old. His response was "what does your age have to do with anything, I think that's a fantastic idea". And with that, I really did continue to enjoy rounding with the team. And they must have enjoyed me too since they asked my professor if I would be coming back. :) And that made me feel real good because I had hoped that I didn't come off as a "know it all", and clearly they didn't think that way. So in the next few days, I'll be setting up a regular schedule to round with Dr.B!!
LIFE IS GOOOD!!!! :)

And that pretty much sums up my half-day rounding in IM at the local county hospital. Absolutely AMAZING, clinical care here I come!!!
Man, where do I begin? I'll start with the obvious; the serious patient risks of not having culturally competent Doctors costs lives, absolutely NO doubt about it! Not only were half of the patients I saw Spanish speaking, they were mostly minority, which probably doesn't come as a surprise considering that most of their funding is from Medicaid/Medicare. So I got a chance to brush off my Spanish speaking skills and my ebonics skills too, LOL!! Honestly, if the Doctor can't communicate with the patient because the translator can't be everywhere at the same time, how in the hell can they effectively provide care?
Anyhoo, during rounds I suggested ordering a Psych eval, thyroid panel, hormone status ie menopause, and a couple other things. And what became glaringly obvious not just to the team that I rounded with but the Attending as well, is that my life, educational, and professional experiences puts me FAR ahead of the average med school applicant in terms of just knowing what to do when what to do isn't obvious. I also think my ability to relate culturally helped too. Sure, my group had me "beat" in many of the clinically obvious things because this is what they've been doing full-time for the last 3 to 5 years. But those basic or gut instinct skills that typically come with age/wisdom, they just didn't have because they haven’t been around long enough or had enough life experience to know anything different. And this is the point older premeds need to emphasize in interviews. All that said, Dr. B my Attending, who's also the professor for my healthcare course, not only speaks fluent Spanish, he's got compassion "on lock". There wasn't ONE patient he didn't easily communicate with and I think that speaks to the kind of person/Doctor he really is.
I almost forgot to mention the computer cart AKA point of care cart, Dr. B used to both review and immediately enter patient data into the EPIC EHR, an image of which is shown below:

Again, I was TOTALLY AMAZED, I had finally seen the EPIC EHR in action in a real life medical setting and it's honectly not as bad as MANY Docs say it is. So the way our rounds worked, is that Dr. B gathered us all around it to discuss the patient, look at labs, xrays, ect. The monitor appeared ot be about 27'. Then we would go see that patient, ask them how they were doing, any complaints, ect, then we returned immediately to the cart to enter the pertinent data. Again, VERY cool!
So after giving me kudos for thinking of differentials on patients that neither he nor the team had thought of, I told Dr. B that I was taking the MCAT in the fall and applying to med school. At almost 50 years old. His response was "what does your age have to do with anything, I think that's a fantastic idea". And with that, I really did continue to enjoy rounding with the team. And they must have enjoyed me too since they asked my professor if I would be coming back. :) And that made me feel real good because I had hoped that I didn't come off as a "know it all", and clearly they didn't think that way. So in the next few days, I'll be setting up a regular schedule to round with Dr.B!!
LIFE IS GOOOD!!!! :)
Wednesday, March 12, 2014
Hell no I won't sign off on this!
And with that statement, I'm now feeling like I have a big ass target on my back as far as my current job is concerned (considering I've been pretty much ordered back into the lab by this coming Monday). Anyhoo, when I ran the Ebola suit suggestion by my Primary Care Doc she essentially said that she will NOT sign off on me wearing that in the lab, even if I do have on an Ebola suit. And there's a damn good reason she said this and I can't get into why that is here. Suffice it to say that my Doctor clearly isn't stupid enough to risk me working in there for fear of being sued should something else go wrong.
So today I work at a leading cancer center. Who knows what tomorrow is going to bring.........................................
In other FAR more appealing news, tomorrow morning I head to county hospital which treats indigent patients for my Internal Medicine rotation and I can't wait! :) As soon as I have time, I'll be sure to update my experiences. And I have a feeling that I'm going to have a LOT more free time in my life soon at least until my next blessing comes along! ;)
So today I work at a leading cancer center. Who knows what tomorrow is going to bring.........................................
In other FAR more appealing news, tomorrow morning I head to county hospital which treats indigent patients for my Internal Medicine rotation and I can't wait! :) As soon as I have time, I'll be sure to update my experiences. And I have a feeling that I'm going to have a LOT more free time in my life soon at least until my next blessing comes along! ;)
Friday, March 7, 2014
May I help you ma'am?
The elderly woman I saw earlier today wandering the halls of the surgical oncology (surg onc) floor just broke my heart. I could tell she had been crying recently and was lost so I offered to help her find her husband in the recovery area even though I still get pretty lost myself.
It turns out that lately, I've been spending a LOT of time with one of my sista' mentors (that I'm trying to convince to apply to med school) because she's considered one of the organizational experts in pathology informatics. And she works on the surg onc floor, so it was her office I was leaving when I ran into the lady looking for her husband.
So just as the lady and I were about to get SUPER lost, my sista' mentor appeared and offered to help both of us find our way. And that meant that I had an unofficial tour of the surg onc recovery area. Well, you can probably imagine "how in the right place" that felt for me as I was looking for the woman's husband. The patient's wife had forgotten almost everything about her husband and could barely speak except to say his name. And I'm pretty sure that the Doc probably talked so far over her head that whatever she did understand was likely quite overwhelming based on the seriousness of what brought her husband to this facility in the first place.
When we finally found her husband she was so thankful and it became obvious that she and her husband were there alone. And that's real sad because I'm certain the wife was pushing 75 or 80. Easy. At any rate, it felt good to be able to help someone who obviously needed it. But I think meeting this woman and being in the recovery area did far more for me than I did for her. And the next time, I'm going to be SURE to get the name of the person I'm offering to help. Because little details like that help people feel so much better!
And this experience reminded me that if I didn't work where I do now, I wouldn't have the opportunity to have these kinds of VERY rewarding experiences. And as tough as it can be to deal with life's challenges like those I'm experiencing on the job now, the rewards are that much better. But more than that, it's absolutely WON-DER-FUL to have a constant reminder of my ultimate career goals!
It turns out that lately, I've been spending a LOT of time with one of my sista' mentors (that I'm trying to convince to apply to med school) because she's considered one of the organizational experts in pathology informatics. And she works on the surg onc floor, so it was her office I was leaving when I ran into the lady looking for her husband.
So just as the lady and I were about to get SUPER lost, my sista' mentor appeared and offered to help both of us find our way. And that meant that I had an unofficial tour of the surg onc recovery area. Well, you can probably imagine "how in the right place" that felt for me as I was looking for the woman's husband. The patient's wife had forgotten almost everything about her husband and could barely speak except to say his name. And I'm pretty sure that the Doc probably talked so far over her head that whatever she did understand was likely quite overwhelming based on the seriousness of what brought her husband to this facility in the first place.
When we finally found her husband she was so thankful and it became obvious that she and her husband were there alone. And that's real sad because I'm certain the wife was pushing 75 or 80. Easy. At any rate, it felt good to be able to help someone who obviously needed it. But I think meeting this woman and being in the recovery area did far more for me than I did for her. And the next time, I'm going to be SURE to get the name of the person I'm offering to help. Because little details like that help people feel so much better!
And this experience reminded me that if I didn't work where I do now, I wouldn't have the opportunity to have these kinds of VERY rewarding experiences. And as tough as it can be to deal with life's challenges like those I'm experiencing on the job now, the rewards are that much better. But more than that, it's absolutely WON-DER-FUL to have a constant reminder of my ultimate career goals!
Beware of laboratory hazards! Especially the human ones!
I don't have words for how happy I am that this week is finally over!! Yeah me! But it basically ended with what I'm now fairly sure is the fact that employment wise, I need to Seek. Life. Elsewhere. And I'm cool with that.
The bottom line is that I'm expected to wear something like the following so that I may be able to work in the lab again with the venting chemical tank. The same type of venting chemical tank that blew up in another research lab a few years ago, but I digress. Here's my new work gear:
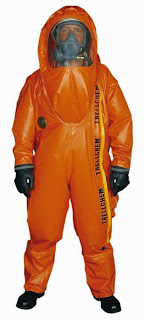
When I was presented with my new lab work attire, I chuckled out loud and asked "where's the Ebola"? That got a laugh out of the HR and ADA reps, but the person over my new and old Supv's didn't find it so funny. Her bad, LOL!! However, they know DAMN WELL that's it's going to be DAMN NEAR IMPOSSIBLE for me to work comfortably or efficiently in the lab at the bench, hood, or at my desk which is also now being relocated back near the venting chemical tank. So I translated all that to mean that what they're really saying to me without directly saying it is this: "we really don't want to work with your Black a$$ anymore, so please get da' hell on". Because I know as a Chemist for the last 20 years that the chemical being vented from the tank doesn't require anything close to this and I know this because over the years I've worked in chemistry and pathology labs with far more dangerous chemicals, that nothing remotely like this is required. OTOH, I've NEVER worked in such close proximity to/or around such a substantially large volume of a chemical like this either. And when I say large volumes, I mean tanks like these in a space around 450 square feet in area:

And yes, there are TWO of them almost as tall as I am (and I'm almost 5'8").
So allow me to be clear, my primary "issue" isn't that I'll have to work in a room with this thing on, people do it every day (for a hellva LOT more money than I'm making). My primary issue today is the same when this all started, the lab skills/safety challenged person charged with running the lab. Put another way, this individual is the ~ 3rd person in an almost 25 year lab career whose presence in the lab scares me $hitless. The fact that it doesn't really vent, it SPILLS air on a regular basis in such a small, averagely vented space is my second concern. The third and most important is the location of the tanks near the ONLY way into/out of the lab. If these tanks were to blow there's a damn good chance that the ONLY entry/exit into the lab would be blocked. Yet I was told today that basically, "too bad for you put on your "Ebola suit", this is what you're going to have to work with". So, I'm praying REAL HARD that God removes me from this situation ASAP and ask that you pray for me too. Fortunately for now, I haven't been ordered back into the lab soon because I need to run this by my Doc (and probably a lawyer too) to get some consensus about what I really need to wear in the lab or if I should be in there at all. In the meantime, I'm applying for jobs just like I don't have one...........................
Moving on, I had the most amazing week to date in my clinical healthcare class!! Whilecramming/reviewing for my midterm this past week (I got an "A" on my exam), I gained more insightful revelations about a couple clinical medical specialties. And again, I'm SO excited that pretty much any clinical specialty is a realistic consideration for me now that my kid is almost an adult. I went through iterations of becoming a Psychiatrist, Intensivist, or just a regular ol’ Family Doc this week. And this reminds me of the stories I’ve heard over the years from third year med student about what they think as they’re doing their clinical rotations. So for my first rotation, I’m going to be at the local county hospital working with the very population of folks, poor, minority, hispanic, I hope to serve one day as a Physician. In fact, it isn’t lost on me that I could end up as a student, Resident, or Attending, at this very hospital one day! :)
The bottom line is that I'm expected to wear something like the following so that I may be able to work in the lab again with the venting chemical tank. The same type of venting chemical tank that blew up in another research lab a few years ago, but I digress. Here's my new work gear:

When I was presented with my new lab work attire, I chuckled out loud and asked "where's the Ebola"? That got a laugh out of the HR and ADA reps, but the person over my new and old Supv's didn't find it so funny. Her bad, LOL!! However, they know DAMN WELL that's it's going to be DAMN NEAR IMPOSSIBLE for me to work comfortably or efficiently in the lab at the bench, hood, or at my desk which is also now being relocated back near the venting chemical tank. So I translated all that to mean that what they're really saying to me without directly saying it is this: "we really don't want to work with your Black a$$ anymore, so please get da' hell on". Because I know as a Chemist for the last 20 years that the chemical being vented from the tank doesn't require anything close to this and I know this because over the years I've worked in chemistry and pathology labs with far more dangerous chemicals, that nothing remotely like this is required. OTOH, I've NEVER worked in such close proximity to/or around such a substantially large volume of a chemical like this either. And when I say large volumes, I mean tanks like these in a space around 450 square feet in area:

And yes, there are TWO of them almost as tall as I am (and I'm almost 5'8").
So allow me to be clear, my primary "issue" isn't that I'll have to work in a room with this thing on, people do it every day (for a hellva LOT more money than I'm making). My primary issue today is the same when this all started, the lab skills/safety challenged person charged with running the lab. Put another way, this individual is the ~ 3rd person in an almost 25 year lab career whose presence in the lab scares me $hitless. The fact that it doesn't really vent, it SPILLS air on a regular basis in such a small, averagely vented space is my second concern. The third and most important is the location of the tanks near the ONLY way into/out of the lab. If these tanks were to blow there's a damn good chance that the ONLY entry/exit into the lab would be blocked. Yet I was told today that basically, "too bad for you put on your "Ebola suit", this is what you're going to have to work with". So, I'm praying REAL HARD that God removes me from this situation ASAP and ask that you pray for me too. Fortunately for now, I haven't been ordered back into the lab soon because I need to run this by my Doc (and probably a lawyer too) to get some consensus about what I really need to wear in the lab or if I should be in there at all. In the meantime, I'm applying for jobs just like I don't have one...........................
Moving on, I had the most amazing week to date in my clinical healthcare class!! While
Sunday, March 2, 2014
Doin' it Cowgirl style!!

* My Cowgirl hat, complete with Tiara, ROTFL!!!
Last Friday at work, many people came in wearing cowboy/cowgirl gear in celebration of the rodeo being in town (did I say that right, LOL??) But I hadn't purchased cowboy anything yet so I didn't participate. Yesterday, I had every intention of going to work for a few hours then going to the rodeo which was only a few blocks away. But once I parked my car and smelled the bar-b-q being cooked from 6 blocks away, I passed on that idea and headed stright for the rodeo! Yummy!

Being a North Carolina girl (by way of Cali), I KNOW good bar-b-q when I taste it. And being the extraordinary southern cook that I am, I can make a mean bar-b-q sauce myself. ); But this Texas bar-b-q is different, owing to it's Mexican influence. And for the most part it's a big FAIL for me because I prefer bar-b-q without the salsa influence. But the free bar-b-q they were serving at the rodeo was quite delicious! I also had a super long corn dog and a funnel cake with a TON of sugar, which means that all I ate for lunch today was a bananna. :(
Overall, it was a good day, nice and cool weather wise, full of friendly people and great food! I heart Texas!!!
Yeeeeee-haaaaaaawwwwww!!! :)
Saturday, March 1, 2014
Natural hair, don't care!!

Over the past few years, I've become known to family and friends for going from wearing a wig (see my "about me" pic) to wearing my natural hair. And I've recently decided to not only wear my natural hair more often, but grow it out very long the way I wore my hair when I had a perm.
Ironically one of the first things I noticed about Black women in Texas is that very few of them wear their natural hair which coming from the East Coast/Metro DC, is VERY strange to me. You would think the opposite would be the case especially in a place where during the month of August, having 100+ degree days for the entire month is not unheard of. And I know from personal experience, wigs are hot as hell in the summer months!
Movin' on, after learning yesterday that my assignment to a new Supv is temporary, I've decided to jump ship as soon I can to another cancer research group. That is unless my department decides not to do that and that's a real possibility given that everything in my department is in such a flux. My readers may also have noticed that I haven't mentioned the type of cancer I'm studying and that's because of the politically charged nature of it at my current institution. Whoda' thunk that political game playing would play such a STRONG role in the quest to "cure cancer". But it does. It really, really does and that in my mind ends up costing lives.
I'll also finally be starting my clinical rotations for my health informatics course and that is so SUPER DUPER exciting, that I can hardly contain myself!! I'm starting with Internal Medicine which is ironically the field of medicine I feel most likely to pursue after med school. I'll also be shadowing my prof and I'll probably let him in on my "secret" to pursue med school after finishing my PhD. And no, I'm not worried about what he's going to say about it, in fact, I don't really give a $hit what he thinks about it. I'm just that laser focused after MANY years in the premed game.
So I think I now have not just a plan for completing this dual degree program, but a GOOD PLAN THAT FITS MY LIFE AT THIS POINT. And I think that's an important distinction to make for a nontrad premed. So here goes my year by year plan:
Summer/August 2014 - Take MCAT
Fall 2014/Spg 2015 - PhD courses
Fall 2015/Spg 2016 - PhD courses
Summer 2016 - Apply to Med school
Fall 2016/Spg 2017 - PhD Courses/Finish PhD
Summer 2017 - Matriculate in Med school
And this is my "worst case" plan, my first choice plan is to apply to med school in the summer of 2015 but wanted to give myself some wiggle room due to some other personal plans I have on the table.

The other highlight of my week was the rooster in the above photo that kept me from getting into my car the other day. I have NO IDEA where this thing came from because there aren't any farms nearby. And I didn't think roosters could fly all that well so how he got here is my lingering question. Needless to say, this thing scared the hell outta' me and it took about 15 mins for to get into my car because he was chasing me around the car. And I'm certain I looked like a fool running away from a rooster. URGH, LOL!!!
Subscribe to:
Posts (Atom)